Polio Switch – What you should know!
If you are a health worker, you must probably be knowing about the WHO project to replace trivalent oral polio vaccine to bivalent polio vaccine also called the ‘Polio Switch’ . It is considered as one of the major and critical step in the eradication of polio from the world.
Oral polio vaccine (aka Sabin) was developed in the 1950s, and has helped take the world to the edge of polio eradication. The active polio cases reduced from >300,000 in 1980 to <10 today. It has been a monumental achievement in public health.
 What is The Polio Switch?
What is The Polio Switch?
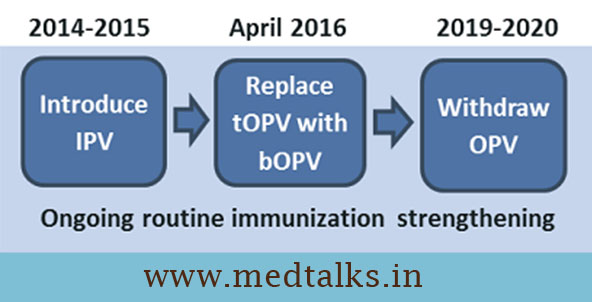
The oral polio vaccine which is in use at present is a trivalent vaccine (tOPV) containing 1, 2 and 3 polio strains. For a while now, the P2 component of the vaccine has caused more problems than it has solved, and has actually resulted in a relatively small number of cases of paralysis. It is also established by various surveys and studies that the cases due to P2 strain of vaccine are non existing for quite some time. So by May 1, all countries that use the trivalent oral polio vaccine must stop administering the current formula and replace it with a new version which contain only strain P1 and P3 and is bivalent (bOPV). The unprecedented synchronized campaign, over 18 months in the planning, is appropriately known as “the switch.”
Risks and Impact of Switch!
The switch does not come without risks. There are three strains of polioviruses. The new vaccine will not have a component that protects against Type 2. Mostly that’s not a problem — P2 strain haven’t been seen since 1999 and have been declared eradicated. After the switch, infants in some parts of the world won’t have any protection against P2 and if there are any Type 2 vaccine viruses left in the environment, or if they are unleashed by the unauthorized or unwitting use of stocks of the trivalent vaccine (tOPV), those children could become infected and crippled. The Global Polio Eradication Initiative, a public-private partnership that includes the CDC and the World Health Organization, has prepared for that possibility, stockpiling vaccines that could be used to control an outbreak if the need arises. Due to this risk, the trivalent polio vaccine should be considered as bio-hazard and must be discarded at all the healthcare centres where it has been used till now.
In India, April 25th is the National Polio switch day. All remaining tOPV vaccine must be discarded and destroyed in proper manner.
Next Step:
By May 1, 2016 all tOPV will be switched to bOPV. From now on in a stepwise manner there is a plan to withdraw OPV once the eradication of polio will be confirmed all over the world. In addition to fixing the Type 2 vaccine virus problem, the switch will serve as a dry run for further down the road, when all oral vaccine use must stop. Once it appears that polio transmission has ceased, the oral vaccine must be discontinued to ensure vaccine viruses also disappear.
Over the two weeks of the switch, thousands of program monitors will be checking hospitals, clinics, and other venues where oral polio vaccine is given to ensure any remaining supplies of the old vaccine are removed from the supply chain and rounded up for safe disposal.